

Background: There is a 2-3-fold excess of both monoclonal gammopathy of undetermined significance (MGUS) and multiple myeloma (MM) among African Americans (AAs) compared to non-Hispanic whites (NHWs) for unknown reasons. It is unclear if risk of progression from MGUS to MM is similar across racial/ethnic groups. We identified MGUS patients and controls from the Multiethnic Cohort (MEC), a population-based cohort study in Los Angeles and Hawaii, described characteristics of and examined risk factors for MGUS among different racial/ethnic groups.
Methods: A total of 637 MEC participants with a diagnosis of MGUS by CMS billing codes and 1,065 race/ethnicity-matched MM-free and presumed MGUS-free controls were identified. Screening for monoclonal proteinemia was performed at the USC Clinical Laboratories using serum protein electrophoresis (SPEP) with reflex to immunofixation (IFX) when SPEP was abnormal. For this study, MGUS was defined as IFX positive with M-protein concentration< 3g/dL. Controls were SPEP- and IFX-negative with no history of MGUS or MM. MGUS cases who progressed to MM during a mean 8.11-year follow-up were identified by linkage with the SEER databases of the Hawaii Tumor Registry and the California Cancer Registry. Multivariable logistic regression was used to estimate odds ratios (OR) and 95% confidence intervals (95% CI) for the effect of body mass index kg/m2 (BMI), diabetes or aspirin use prior to diagnosis on the risk of MGUS and progression to MM.
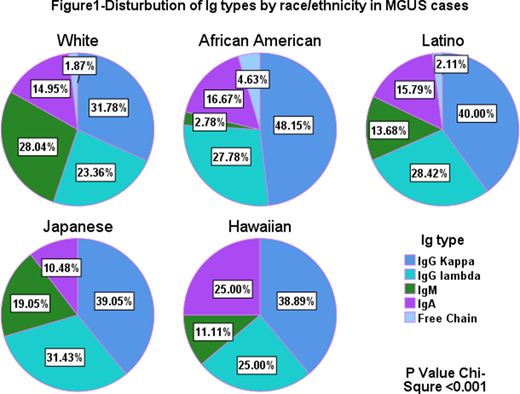
Results: A total of 452 participants had laboratory validated MGUS. The racial/ethnic distribution was 109 AAs, 107 NHWs, 95 Latinos, 105 Japanese and 36 Hawaiian's. 58.6% were males. From the pool of laboratory-validated controls, an equal number of controls were frequency matched to cases by race/ethnicity, age and sex. Mean age at blood draw was 65 years for Hawaiians, 69 years for NHWs and Latinos, and 70 years for AAs and Japanese. The distribution of immunoglobulin (Ig) isotypes differed significantly by race/ethnicity(p=0.001) (Figure 1), with AAs having the highest proportion of IgG Kappa (48.1%) and the lowest proportion of IgM (2.8%) compared to other racial/ethnic groups (range IgG Kappa 31.8%-40%, range IgM 11.1%-28.0%). There was no difference in isotype distribution by sex (p=0.28). AAs and NHWs had the highest (mean=0.75 mg/dL ±0.6) and lowest (mean=0.53 mg/dL ±0.6) levels of M-protein, respectively, but there was no significant difference when all racial/ethnic groups were compared. Each unit of BMI (kg/m2) was associated with a 16% increase in risk of MGUS among Hawaiians (95% CI= 1.04,1.30); and a borderline increased risk ranging from 2%-7% among the other racial/ethnic groups. Neither history of aspirin use nor diabetes mellitus were significantly associated with MGUS risk.
A total of 109/452 MGUS patients progressed to MM between 1 to 10 years after blood draw. Compared to NHWs, AAs (OR=2.09; 95%CI= 1.08-4.05) and Latinos (OR= 2.55, 95% CI=1.29-5.08) were more likely to progress. Progression was not significantly associated with sex (p=0.34) or BMI (p=0.12). Progressors were slightly younger than non-progressors (-1.6 years, p=0.057). A higher risk of progression was associated with IgA compared to IgG Kappa (OR=2.45; 95% CI=1.34-4.48) and an M-spike >1.5 g/dL compared to <1.5g/dL (OR=5.81, 95% CI=2.92-11.57). IgM was associated with a lower risk of progression (OR=0.03, 95% CI= 0.00-0.23).
Conclusion: The distribution of MGUS isotypes and risk of progression to MM differed by race/ethnicity, with AA and Latinos more likely to progress, not explained by age at blood draw. Because we detected prevalent MGUS, lead time bias could explain racial/ethnic differences in risk. More studies with diverse populations and large sample sizes are needed to better understand the disparities in MGUS risk and progression, along with the underlying biological explanations.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal